Urology Research: Diversity in Prostate Cancer
Author:
Jennifer Bepple, MD, clinical advisor, Verana Health
The following real-world data analysis of the American Urological Association (AUA) Quality Registry (AQUA) was featured in the March 2023 issue of AUANews. More real-world urologic research leveraging the AQUA network of more than 2,000 healthcare providers, nearly 10 million patients, and 9 years of longitudinal data can be found here.
Racial representation in Prostate Cancer Care: An AQUA Registry Analysis
By: Jennifer Bepple, MD; Marie Humbert-Droz, PhD; Junlin Jiang, PhD; Daniel Lee, MD, MS
Race is a known risk factor for prostate cancer. Black men are more likely to present with prostate cancer at a younger age with more aggressive disease than White men, with more than 2-fold higher rates of metastatic disease at diagnosis. These racial disparities may have deepened during the COVID-19 pandemic, as Black men were significantly less likely to receive surgical treatment for prostate cancer.
Understanding the relationship between race and treatment patterns for prostate cancer is important in discussions around outcomes and promoting equitable access to health care.
Understanding the relationship between race and treatment patterns for prostate cancer is important in discussions around outcomes and promoting equitable access to health care. In collaboration with Verana Health, we evaluated the racial diversity of unique patients identified to have prostate cancer in the national AUA Quality (AQUA) Registry from January 1, 2012 to February 27, 2022.
Over the 10-year study period, we identified 495,460 patients with prostate cancer, as defined by the presence of an ICD (International Classification of Diseases) code for prostate cancer and at least 1 Gleason score found within electronic health record documentation. We also linked claims data with registry data (Komodo Health, Inc) to ensure adequate coverage of treatment types within our patient population. In this cohort, 77.7% of patients were found to have a self-identified race, with the remaining 22% missing racial demographic information. Of those included in the prostate cancer cohort, 64% were White, 11.8% were African American, 1.1% were Asian, and <1% were identified as “other”.
When evaluating the AQUA data registry, we found similar treatment patterns stratified by race.
When evaluating the AQUA data registry, we found similar treatment patterns stratified by race. There were similar proportions of men undergoing androgen deprivation therapy; 29.8% of White, 30.3% of African American and 32.2% of Asian patients underwent androgen deprivation therapy. For external beam radiation therapy, the proportions of patients were found to be, 21.2%, 22.8% and 22.5%, respectively. For radical prostatectomy, 22.9% of White, 18.5% of African American, and 18.9% of Asian patients underwent a prostatectomy (Figure 1).
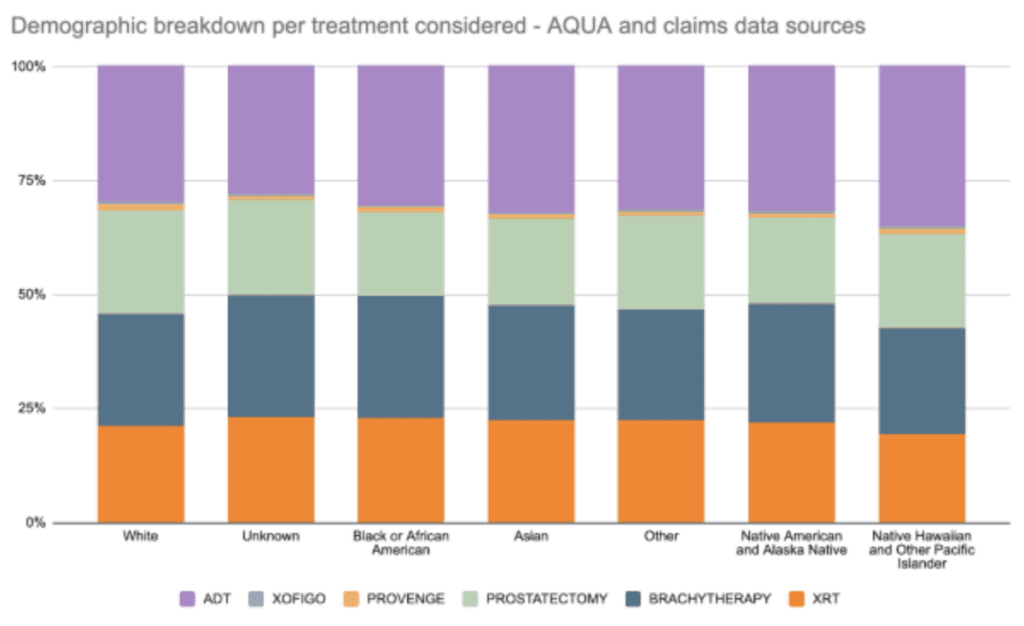
When analyzing select treatments for advanced prostate cancer, sipuleucel-T (Provenge) infusion and radium Ra 223 dichloride (Xofigo), there was a decline in the number of treatments between 2020 and 2021 across all races. This coincided with the peaks and troughs of the COVID-19 pandemic and patterns of access to care. This decline was equally distributed across all races.
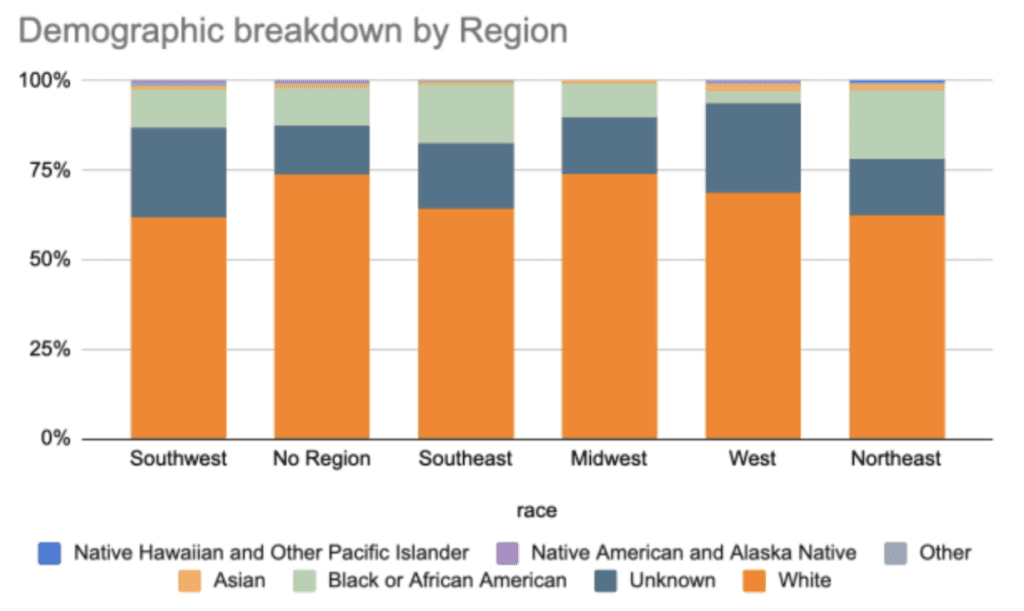
Our findings highlight some of the pitfalls and potential of electronic health record-based real-world data. The challenge of missing patient demographic information such as race is not unique to the AQUA data set. Publications in other practice specialties have similarly shown one-quarter or more of patients who lack this key demographic data. Within the AQUA data set, the missingness of race was associated with geographic region, with the Southwest and Western regions having the highest percentages of unknown racial data (Figure 2).
It is worth noting that the percentage of unknown race per year within AQUA for all considered treatments decreased from 20.8% (2017) to 15% (2022). This suggests that documentation has increased over time, but there remains room for improvement.
Given that race is a well-established risk factor for prostate cancer and other health conditions, these findings present an opportunity for clinicians to ensure demographic information is captured accurately, and exploring ways to accurately impute this information when it is not. It is worth noting that the percentage of unknown race per year within AQUA for all considered treatments decreased from 20.8% (2017) to 15% (2022). This suggests that documentation has increased over time, but there remains room for improvement.
Citations:
- Yamoah K, Lee KM, Awasthi S, et al. Racial and Ethnic Disparities in Prostate Cancer Outcomes in the Veterans Affairs Health Care System [published correction appears in JAMA Netw Open. 2022 Feb 1;5(2):e222773]. JAMA Netw Open. 2022;5(1):e2144027. Published 2022 Jan 4. doi:10.1001/jamanetworkopen.2021.44027
- Bernstein AN, Talwar R, Handorf E, et al. Assessment of Prostate Cancer Treatment Among Black and White Patients During the COVID-19 Pandemic. JAMA Oncol. 2021;7(10):1467-1473. doi:10.1001/jamaoncol.2021.2755
- Fernanda C G Polubriaginof, Patrick Ryan, Hojjat Salmasian, Andrea Wells Shapiro, Adler Perotte, Monika M Safford, George Hripcsak, Shaun Smith, Nicholas P Tatonetti, David K Vawdrey, Challenges with quality of race and ethnicity data in observational databases, JAMIA. 2019; 26(8-9): 730–736.
- Branham DK, Finegold K, Chen L, et al. Trends in Missing Race and Ethnicity Information After Imputation in HealthCare.gov Marketplace Enrollment Data, 2015-2021. JAMA Netw Open. 2022;5(6):e2216715.

Let's Accelerate Research Together
To learn more about Verana Health, please fill out the information below and our team will follow up with you as soon as possible.

{kind=link}